Tracy Swan is travelling to a wedding in Kenmore when she gets the phone call every parent dreads.
Spinning the car around near Dunkeld, Tracy races to Perth Royal Infirmary.
Jodie is on life-support. The outlook is not positive.
Five days later, on May 22 2013, the machine is turned off.
“She never should have had the chance to do what she did”, Tracy mourns.
The health board was fined £120,000.
This death, nor details of the person involved nor how they died has ever been made public.
Murray Royal Hospital: State-of-the-art facility
 Murray Royal Hospital opened its doors in June 2012 – sold as a £75 million state-of-the-art mental health facility it has become a looming presence on the Kinnoull hillside above the Fair City.
Murray Royal Hospital opened its doors in June 2012 – sold as a £75 million state-of-the-art mental health facility it has become a looming presence on the Kinnoull hillside above the Fair City.
Located within its walls is Moredun – a general adult psychiatry (GAP) ward for male and female patients aged 18 – 65 suffering from acute mental health disorders.
Originally a 30-bed ward, now reduced to 22, Moredun was designed to look after the most vulnerable in society.
But when First Minister Alex Salmond officially opened Murray Royal a year later in June 2013, Jodie McNab was already dead.
By January 2021 four more patients had died.
How did these tragedies occur in a facility where keeping patients free from harm, from self-harm, was of paramount importance?
TRIGGER WARNING: THE FOLLOWING INVESTIGATION GIVES DETAILED ACCOUNTS OF SUICIDE WHICH SOME READERS MAY FIND DISTRESSING
Jodie McNab, a former Dunning and Perth Academy student, had a history of self-harm and attempted suicide stemming from abuse she suffered as a child.

Her mum Tracy noticed a change in her daughter from Primary Seven but it wasn’t until years later she understood why.
“Before all that, she was really happy, really good, really popular at school – done well with her work,” said Tracy.
Due to her experiences, Jodie had been admitted to Murray Royal Hospital on a number of occasions.
In 2010, during three separate admissions to the former facility, Jodie had attempted to hang herself on each occasion.
Then, in February 2013, Jodie was discovered in her room at the new Murray Royal with an item tied around her neck which she was attempting to secure to her bed.
Four months later, at 1.10pm on May 18 – on the day her mum was travelling to a wedding in Kenmore – Jodie was found in her room with the same type of item tied around her neck secured to her bed.
Staff caring for Jodie that day were unaware of the February attempt on her life.
Murray Royal Hospital records were ‘appalling’
“What they had in writing (records) for Jodie was appalling,” says Tracy.
“A lot of the things that Jodie had done they hadn’t told us about – we were finding out at different stages through the inquiry, through our solicitors, through the fiscal.”
Tracy remains angry over a number of issues leading up to her daughter’s death.
The mum questions why her daughter, who was sectioned following a self-harm event 10 days earlier, was allowed access to the item she used to take her life.
“Why was she not allowed her phone charger but was allowed (that item)?” asks Tracy.
“She took her life with an (item) she shouldn’t have been allowed on.”
Jodie died after securing the item to a ligature point on her bed – a Kings Fund bed to be specific.
NHS Tayside already knew the dangers associated with Kings Fund beds as they had been involved in the death of another patient through hanging nearly six years previous.
On September 8 2007, Michael Dodds took his life in Carseview, Dundee, by attaching an item to a ligature point on a Kings Fund bed.
During the following Fatal Accident Inquiry in August 2009, Sheriff Derek Pyle questioned why the beds were still being used in Carseview.
He said: “The issue of what is a suitable replacement for the Kings Fund beds is not an easy one, but I am still astonished that after so much time the health board seems no nearer reaching a final decision.”
Despite these concerns, NHS Tayside purchased 52 Kings Fund beds for Moredun Ward in 2012.
It is understood that around 20 of those beds remained on Moredun until December 2015.
‘Three weeks later she was dead’
Rebecca Sangster arrived in this world a few days before Christmas Day 1983. She and brother Tom were the first set of twins born at Peterhead College Hospital in 20 years.

The family moved to Abernethy, Perthshire, in early 1988 where the young Rebecca spent a happy and active childhood, joining the Brownies and Guides and taking up judo and mini-curling.
As she grew older, Rebecca developed a passion for jewellery creation.
She was named student of the year for jewellery studies at Lauder College in Dunfermline before completing a HND in jewellery design at Springburn College near Glasgow in 2015.
The 31-year-old was in the process of setting up her own business when she was admitted to Moredun Ward in early October of that year.
Three weeks later she was dead. She had taken her life after securing an item to a wardrobe door in her room.
Rebecca enters Moredun Ward after a significant self harm event.
Rebecca is found with a ligature around her neck.
Rebecca is found again with a ligature around her neck.
Rebecca is found with that same type of item dangling around her neck.
She is rushed to Perth Royal Infirmary but never regains consciousness.
Rebecca Sangster is pronounced dead. She was 31 years-old.
‘A pattern of behaviour’
Ann Sangster, Rebecca’s mum, is clear – her daughter’s death was not an unavoidable accident.
She believes the whole culture on the ward was to blame.
“My family were seriously concerned with regards to NHS Tayside’s practice on patient care and wellbeing, the duty of care,” says Ann.
She said “there also appeared to be no appropriate supervision or accountability” for staff to maintain and ensure an appropriate standard of care.
Concerns regarding patient care and accountability were raised by numerous people contacted by this investigation.
“These are not tragic single errors but a pattern of behaviour that is dangerous,” said Ann.
She claimed “a tolerance of poor standards” placed vulnerable people at risk.
This pattern of issues is clear in the reporting and recording of serious incidents.
NHS Tayside employs an electronic DATIX system to record such events which are then flagged to service managers to trigger a review.
However, many incidents were just simply never recorded.
According to The Crown, in May 2013 there were two attempted suicides by a patient using a ligature attached to the wardrobe doors – neither was recorded on the DATIX system.
In March 2015, another two suicides were attempted using the wardrobes – only one was reported to the DATIX system and was filed without important information.
In total, between May 2013 and November 2015, only 10 attempted or completed suicides using ligature points were filed using the DATIX system.
The deaths of Jodie and Rebecca, using ligature points, were never recorded in DATIX.
Self-harm – a ‘negligible’ event
In addition to flagging, or failing to flag, incidents on the DATIX system, Moredun staff were asked to grade the seriousness of such events.
The grading system was in itself a problem.
Green would be used for negligible incidents.
Yellow was used for minor events.
…whilst major adverse events were to be filed as red.
Under the guidance for the system, self-harm was to be treated as a green, or negligible event…
…while suicide was a red event.
There was no guidance on how suicide attempts should be reported.
No reviews were triggered before the deaths of Rebecca and Jacqueline Proctor in late 2015.
Reports ignored in Moredun Ward
Jacqueline Proctor was an accomplished artist and support worker for the mental health charity Plus Perth when she entered Moredun Ward voluntarily on October 8 2015.
The 60-year-old had been admitted to Murray Royal Hospital numerous times before.

She had a close relationship with her son who came to visit her daily at the hospital.
During his visit on November 3, he noted that his mother was withdrawn, confused and upset.
The following morning, at 8.05am, a member of staff entered Jacqueline’s room and found her hanging from the door of her en suite bathroom.
Her death was confirmed at 8.38am.
The en suite bathroom doors had been flagged in a report published in October 2013 following the death of Jodie McNab.
The report stated that a patient had attempted to use them as a ligature point and recommended they be removed and replaced with magnetic privacy curtains that had been installed at Carseview.
The report was circulated to the then director of mental health Jim Crichton, director of operations Ken Armstrong, and interim service manager Grace Gilling.
No action was taken to replace the bathroom doors at that time.
NHS Tayside said it does not comment on matters relating to individual members of staff.
Former director of mental health Jim Crichton apologised to the family of Jacqueline Proctor when he was contacted by this investigation.
“The loss of any patient through suicide is devastating for the family and everyone involved in their care,” he said.
“I deeply regret that Ms Proctor was able to take her life utilising the bathroom door in what should have been a safe environment.
“I apologise to Ms Proctor’s family that the recommendations regarding removal of the bathroom doors in the newly built Moredun Ward was not put in place as it may have prevented this very sad outcome.”
‘Patient safety issues’
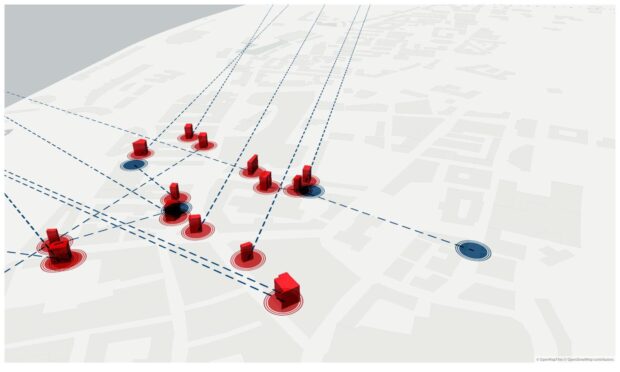
Tracy believed that Jodie had been placed too far away from the nurses’ station.
This is the distance between the two rooms.
Staff needed to walk through more than one set of double doors to visit the room.
NHS Tayside told this investigation: “To improve observation on Moredun Ward, taking into account the layout, staffing levels have been increased, bed numbers have reduced, there is a dedicated floor nurse and mirrors have been installed to increase visibility.”
12.5 hour shifts
NHS Tayside were unable to provide staffing levels and staff to patient ratios for the years between 2013 and 2021.
It is required that there is seven staff on the day shift…
…with one staff member working a “twilight shift”.
In addition, there is a supernumerary full-time senior charge nurse and full-time ward clerk.
The Moredun Ward shift patterns are as follows…
and Twilight Shift: 9pm to 2am
Which gives the following staff to patient ratio at each time period.
A spokesperson for NHS Tayside added: “The nursing team has the flexibility to increase staffing numbers dependant on levels of patient need and activity.
“These decisions are based on knowledge of the patient and staff group and are made at a ward level with the support of the senior and or lead nurse.”
At Perth Sheriff Court in 2020, Sheriff Lindsay Foulis criticised the health board for taking so long to action changes, including staffing.
“It shouldn’t have required three deaths before that very significant review was undertaken,” said the Sheriff.
“It was plagued with chronic staff shortages, up to 50% were off regularly and reliance was placed on agency staff which had an adverse effect on continuity of care.
“The conclusion I’m inevitable drawn to is the culpability of the accused body is high.”
The report by the Mental Welfare Commission also stated after numerous visits that the ward layout problems at Moredun will be resolved when NHS Tayside completes its plan to host all general adult psychiatry admission wards at Carseview.
This investigation understands that the controversial plan is heavily disputed and nowhere near fruition – despite the ‘up to two year’ completion timescale given to the Commission in 2018.
Moredun Ward patients ‘forcibly injected’
Multiple witnesses have described seeing patients being held down and forcibly injected on Moredun.
In May 2013, around the time of Jodie McNab’s death, it was reported that three members of staff were suspended from Murray Royal for refusing to forcibly medicate a patient.
Tracy Swan witnessed the practice with her own eyes.
“You know when you see people getting arrested by police and they’re face down and they get their hands put behind their back to be carried into their room,” she said.
“The patient is screaming and shouting, and they get a jag to sedate them.
“I sat and watched that whole thing and thought it could have been avoided if they had approached that patient properly.”
Another source who witnessed a similar event told The Courier, “It’s what’s happened for years.”
They added: “I would not put any of my family in there (Moredun Ward).”
Investigation ongoing
Celine Dinis’ family are still waiting on the NHS Tayside report that will give them answers about the circumstances surrounding her death.

It has been over a year since she died on January 4 2021.
The health board told this investigation that a senior mental health consultant had met with Ms Dinis’ family in May 2021 to share the findings of their immediate review following her death.
However, the Serious Adverse Event Report (SAER) has still not been completed by the health board.
“The SAER into the death of Ms Dinis is complex and wide-ranging and involves the whole system of care across community and acute services,” said an NHS Tayside spokesperson.
“Therefore, it is taking a significant amount of time to investigate in full and we are sorry for the upset this is causing the family.”
A separate investigation by the Scottish Fatalities Investigation Unit (SFIU) is also ongoing after the Procurator Fiscal received a report in connection with Celine’s death.
A spokesperson for Procurator Fiscal said: “The family will continue to be kept updated in relation to any significant developments.”
Ann and her family waited six months for the findings of NHS Tayside’s Local Adverse Event Review (LAER) into Rebecca’s death.
The report should have taken 28 days.
A further eight months passed before the family received a copy of the Significant Clinical Event Analysis (SCEA) report.
Ann claims her daughter had been dead for 26 months before the family received an apology from NHS Tayside.
The Sangsters now believe that an independent Fatal Accident Inquiry (FAI) should automatically follow the death of an inpatient who was being held under the Mental Health Act.
To date no FAI has ever been carried out into the deaths of Jodie, Rebecca or Jacqueline.
Latest Moredun Ward death ‘set off alarm bells’
Tracy, Ann and the family of Jacqueline Proctor fought for years for answers from NHS Tayside – eventually taking them to court.
The health board promised change and that lessons would be learned.
Celine’s death 10 months after the court case hit them hard.
For Tracy it was too much; Celine and Jodie were the same age. Tracy has been told they were even placed in the same room on Moredun.
Upon hearing the news, the mum said she “broke down massively”.
“I thought, I can’t believe this, they were found guilty in court and now there’s another 22-year-old girl,” she said.
“It was like Jodie’s case all over again. The age, the hospital, the ward, everything.
“It set off alarm bells.
“Obviously I was so sad for the family but I was so angry that this had happened again. Really angry.
“I don’t think they’ll ever learn their lessons, they’ve failed too many people in different ways.”
Ann has similar views on NHS Tayside’s ability to change.
“When I read about the young woman’s death I was very upset for her family, for another lost life and propelled back to that dark stage in my family’s life,” she said.
“I also felt anger followed with disappointment towards NHS Tayside – they had badly let down previous lost people and their families.”
Rebecca’s mum believes that individual staff members will need to speak out if any real change is to be achieved.
“Can things change for the better will be largely dependent upon the integrity of individuals working within the NHS,” she said.
‘NHS Tayside is more interested in protecting its reputation than looking after the interests of its patients.’
By July 2021, of the 49 recommendations for change, NHS Tayside had graded 35 as complete.
The Independent Oversight Group believe the correct number is 9.
… “However we have yet to see evidence of the positive impact on people of their actions.”
Dr Strang’s Trust and Respect report was praised by the people contacted by this investigation – including Ann who took part in the inquiry.
But they are now losing faith that NHS Tayside will ever properly implement its findings.
“We felt confident in David Strang’s initial report and it was hoped this would result in safer care for patients,” explained Rebecca’s mum.
“Our disappointment is that progress appears erratic and very slow.”
There is a shared feeling among families that in their opinion NHS Tayside remains somewhat unaffected by the 2020 court ruling and an anger that no person has been held accountable for the deaths.
Tracy said: “I would love to confront the staff that were on that day with Jodie and were supposed to be looking after her and did not look after her.
“That’s what angers me more – it was the QC for NHS Tayside that was in court.
“It’s infuriating. I feel really angry about it, that not one person has been held accountable for it.”
The last words of this investigation will be left to Ann Sangster.
“We all have mental health; it is our state of wellbeing and can benefit from assistance at times.
“For some on occasion this requires hospitalisation and care.
“Any of us may require this at any stage in our lives.”
NHS Tayside response
A spokesperson for the health board admitted to this investigation that the deaths of Jodie, Rebecca and Jacqueline should never have happened but said improvements had been made to Moredun Ward.
“Tayside Health Board admitted criminal failings in relation to the health and safety of patients that led to the deaths of three patients at Moredun Ward at Murray Royal Hospital in proceedings which concluded in March 2020,” said the spokesperson
“The Board have said it was clear the tragic events at Murray Royal Hospital should not have happened and apologised to families.
“The thoughts of the Board of NHS Tayside remain with the families affected.
“During the legal proceedings in 2020, the court heard there had been a programme of improvements made at the ward and further improvements have been made since.
“Improvements are ongoing and include improvements to both the environment and the patient care pathway.
“A major programme of works was completed in Moredun Ward which focused on removing ligature points from the fixtures and fittings in the ward. Beds, bedroom doors, en suite bathroom doors and bedroom.
“A new protocol for the observation and engagement of patients was introduced in all Mental Health and Learning Disability Wards across Tayside.
“The new protocol was developed with Healthcare Improvement Scotland as part of a new national approach to Improving Observation Practice.
“Moredun Ward team won the inpatient award at the 2021 Mental Health Nurse Forum for Scotland for their work in Improving Observation Practice.
“To improve care planning, the Tayside Mental Health and Learning Disability Nursing Standards for Person Centred Care Plans were developed in 2019 and updated in 2021 following feedback from patients.
“The standards are now referenced in the Mental Welfare Commission Person Centred Care Plans Good Practice Guidance.
“The Moredun team has undergone training in trauma informed practice, safety and stabilisation and decider skills to further enhance patient care on the ward.”
Anyone affected by the issues raised in this article or in need of assistance can call Samaritans free of charge 24 hours a day on 116 123, or by visiting the Samaritans website.
If you would like to speak to our Impact investigations reporter Sean O’Neil please email soneil@dctmedia.co.uk
More Moredun Ward coverage
- Nicola Sturgeon told families are being ‘failed’ at Perth’s Moredun Ward
- Moredun Ward: Mum dismisses Humza Yousaf response to investigation as ‘twaddle’
Read next
Credits
Words by Sean O’Neil
Story design by Cheryl Livingstone
Data visualisations and scrollytelling by Emma Morrice and Lesley-Anne Kelly
Graphics by Mhorvan Park and Gemma Day
SEO by Jamie Cameron